
The Cardiac Borough, Part I: After the Anchor Industry

The Cardiac Borough is a four-part strategic essay series examining how 'the production of cardiometabolic health' can become New York City's next economic export engine, replacing the gravitational role Wall Street has played for a century. Published by Blue Spoon Consulting, the series applies ecosystem-centered market strategy and Hardcore Zen to the question of what happens when healthcare becomes the city's dominant industry.
Before the economics, there is the psychic architecture.
The thing that gets lost first is not the jobs, not the capital, not the GDP per capita or the tax base or the trade balance, all of which eventually follow, all of which are measurable and grievable in the ordinary registers of policy analysis. The thing that gets lost first is identity, the story a place tells itself about what it is for. The self-narration that makes morning feel purposeful, that organizes the relationship between people and their labor, between a city and its function in the world, between an entire civilization and its reason for existing on this particular latitude at this particular moment in history.
Consider what it meant to be from the Ruhr Valley in 1960, when the coal and steel complex that had built modern Germany — that had armed two wars, fueled an industrial miracle, and provided the muscular infrastructure around which an entire European working class organized its identity — was entering its long and irreversible twilight.
Nordrhein-Westfalen had been the workshop of the continent. The Krupp works in Essen, the Thyssen furnaces in Duisburg, the coal shafts running under towns with names that the rest of the world would never learn to pronounce, these were not merely employers. They were the organizing metaphysics of a regional civilization, the answer to the question of what this geography, with its deposits of coal and ore and its inheritance of Protestant industrial discipline, was meant to contribute to the human project. When the mines began closing in the 1960s and the steelworks contracted through the 1970s and 1980s, the Ruhr did not simply lose payroll. It lost its account of itself.
It became, in the phrase that German sociologists would eventually develop for it, strukturschwach — structurally weak — which is the bureaucratic vocabulary for a place that no longer knows why it exists.
Or consider what it meant to be Detroit in 1978. Not just the economic reality of Detroit, the Big Three, the UAW, the highest per-capita income of any major American city in the postwar decades, but the psychic reality of it.
Detroit understood itself as the place where the modern world was manufactured. Not assembled, manufactured. There is a difference, and Detroiters knew the difference, which is why the contempt for foreign competition had in it something almost theological, a sense that the offense was not merely commercial but ontological. The automobile was an American invention. Mass production was an American invention. The forty-hour week, the middle-class wage, the possibility that a man who worked with his hands could own a house and educate his children, these were Detroit inventions, or near enough that the distinction didn't matter to anyone who lived there.
When Japanese and German manufacturers began taking market share in the 1970s, and when the oil shocks restructured the economics of the industry in ways that American manufacturers were too rigid and too arrogant to adapt to, what collapsed was not just the industry. What collapsed was a story about American industrial supremacy that had organized the self-understanding of a city, a region, a class, and, in its way, a nation for the better part of a century.
The jobs were bad enough. The loss of the story was something closer to a civilizational injury.
Narrative Lost
That injury does not stay historical. It recurs, with new protagonists, in the present tense.
Jim Farley, the CEO of Ford, brought a $30,000 Xiaomi EV back from China to Dearborn, a car with a zero-to-sixty time of two seconds, facial recognition, and a level of digital integration that made the products of the company his grandfather had come to America to work for look like they had been designed in a different century, which they had. "It was one of the most humble moments," Farley told The Los Angeles Times this month, "when you realize the earth is shifting competitively under your shoes."
He now keeps a picture of that car in what he calls his metaphoric locker, a daily reminder of what humility feels like when the earth is moving under your feet and the only honest response is to keep moving faster. The man who runs one of the companies that invented the modern automobile, the company that gave the world the moving assembly line, the five-dollar day, the very concept of the affordable mass-market car, carries a photograph of a Chinese competitor's vehicle because that is what it looks like when an industry loses the story it told itself about why it could not be beaten.
Ford lost $4.7 billion on its EV business in 2023, and that widened to $5.07 billion in 2024, driven by pricing pressure and investment in next-generation EVs. Ford is forecasting up to $5.5 billion in losses for 2025. The cumulative tab across just three years: roughly $15 billion.
The psychic architecture of a dominant industry is always, at its deepest level, a story about why its activity matters. Why making steel, building cars, discovering molecules is not just economically necessary but meaningful. It is the story that recruits talent, that sustains effort through difficulty, that provides the motivational infrastructure for the extraordinary human energy that any great industry requires. And when the story becomes untenable, when reality contradicts it persistently enough that even true believers can no longer maintain it, the collapse that follows is not just economic. It is existential.
It is the collapse of meaning.
Even now, in March 2026, The Economist is reporting from Baden-Württemberg — Germany's most patent-intensive state, home to Mercedes, Porsche, and Bosch — that Stuttgart's corporate tax receipts have fallen by nearly half in two years, and that nearly half of voters fear the region could face the fate of Detroit.
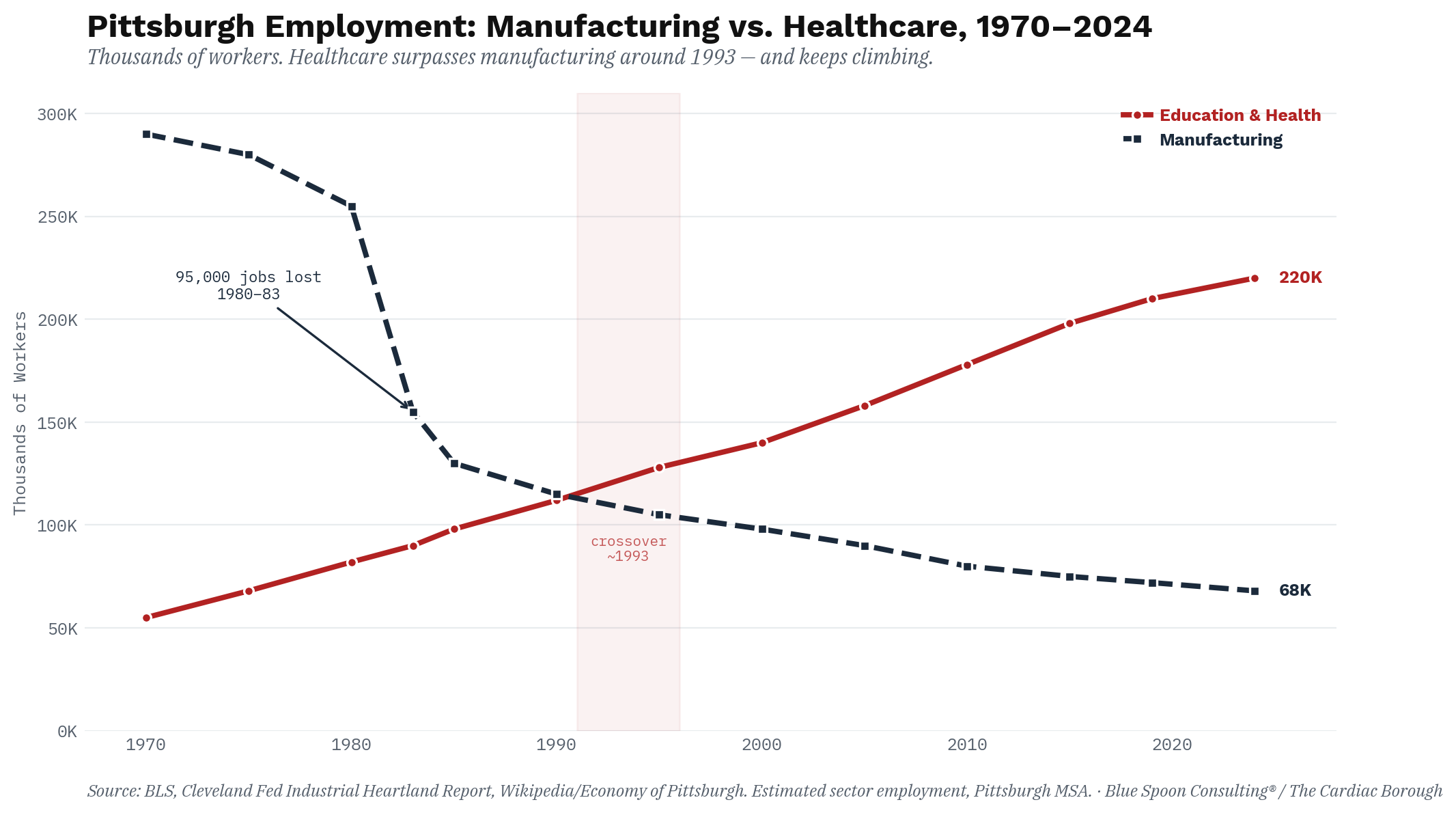
There is a moment, and historians will argue about exactly when it arrives, at which a city stops being the thing it was and begins being something it does not yet have a name for. Pittsburgh hit that moment somewhere between 1979 and 1983, and the way it hit it was not gentle. It was not a managed transition, a strategic pivot, a thoughtful repositioning of civic assets. It was a collapse. The mills went dark the way the human heart arrests, not gradually, not theoretically, but all at once and with a finality that left no room for negotiation.
Between 1980 and 1983, roughly 95,000 manufacturing jobs evaporated from the Pittsburgh region. By the time the twin recessions of the early eighties had run their course, Pittsburgh's employment had contracted by 8.5 percent, more than four times the national decline of 2.2 percent. The mills that had made the city the steel capital of the world, that had at one point produced a third to half of all American steel output, laid off 153,000 workers following the 1981–82 recession alone. Allegheny County shrank by 12 percent between 1950 and the 1990s. An entire civilization of labor — the most powerful industrial union in the history of American capitalism, the men who in 1973 had negotiated what was arguably the most generous labor contract ever won by a blue-collar workforce — simply ceased to exist as an economic force within the span of a single presidential term.
What replaced it was not a plan. It was a biological response.
Pittsburgh's Healthcare Transformation: Accident or Strategy?
The historian Gabriel Winant spent a decade inside this question. His 2021 book The Next Shift traces what happened to Pittsburgh after the mills closed, not as an economic abstraction but as a biological process unfolding in real bodies, real households, real hospital corridors.
The steel industry did not simply close; it produced the conditions of its own successor.
Steelworkers aged. The decades of molten metal and asbestos and physical brutality caught up with them. Their wives and daughters, who had been held to the economic periphery by the masculinized structure of mill employment, entered the healthcare workforce to replace the income the mills had stopped providing. Medicare and Medicaid, which the steelworkers' unions had fought for in part as extensions of the private welfare state they had built through collective bargaining, created enormous blocs of insured patients. The care economy expanded to absorb the human wreckage of the industrial economy's implosion. It was not strategy. It was metabolism.
Today, the largest private employer in Pennsylvania is the University of Pittsburgh Medical Center.
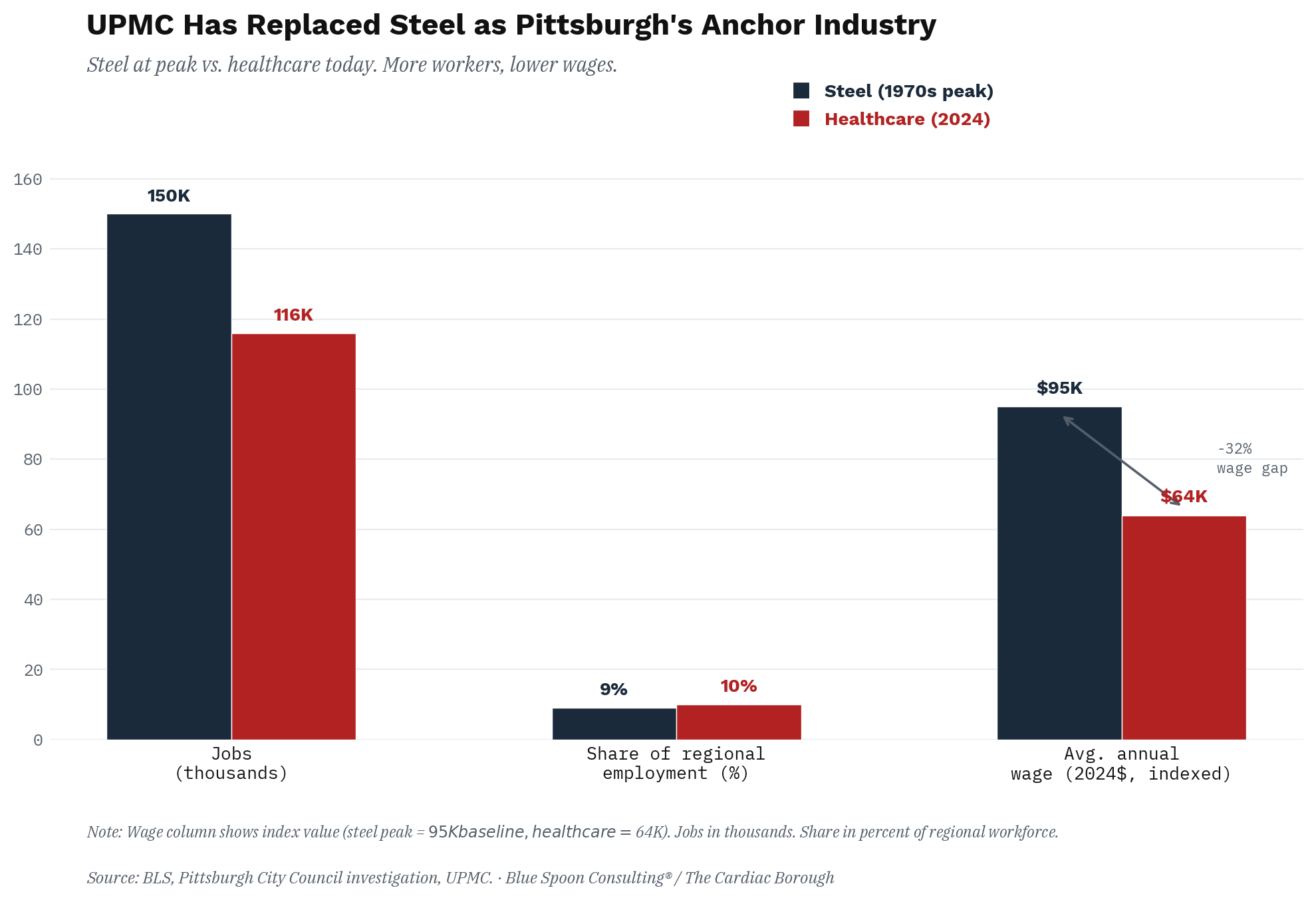
UPMC alone employs more than 92,000 people across 40 hospitals and 700 outpatient sites. All hospital, clinic, and physician employment combined accounts for roughly 116,000 jobs in the Pittsburgh region, approximately ten percent of total regional employment. An analyst noted the historical significance of that figure with the matter-of-fact delivery of someone who has been staring at economic data for too long: healthcare now represents both more jobs and a higher share of regional employment than the steel industry did at its 1970s peak.
The transformation is real. Pittsburgh has been celebrated internationally for it. Barack Obama chose the city for the 2009 G-20 Summit precisely because its reinvention served as a usable narrative, a proof of concept for the proposition that post-industrial America could reconstitute itself around the industries of the mind and the body rather than the furnace and the forge. The Economist consistently names Pittsburgh as one of the most livable cities on the American mainland. Carnegie Mellon produces roboticists. The rivers are clean.
And yet.
The critic in the room, the one who refuses the comfortable story, must notice what Winant noticed: the wages.
The average healthcare support worker in Pittsburgh earns $17.31 an hour. The average steelworker in 1973, at the moment of peak union power, was among the highest-paid industrial workers on the planet. By 1980, the average Pittsburgh production worker in manufacturing earned $360.89 weekly, roughly $70 above both the state and national average. The healthcare economy that replaced it did not replicate that premium. It could not, by structural logic, replicate it, because healthcare is labor-intensive in a way steel was not, which means the fundamental incentive of hospital administration has always been to hold wages down rather than share productivity gains with workers the way unionized industrial employers eventually did.
As Winant told Governing magazine: health care jobs "are done by people who have the least power in the labor market, which has historically been women and people of color."
Pittsburgh traded hardhats for scrubs. The hardhats were better paid.
This is the paradox that haunts the post-industrial healthcare economy everywhere it has taken root, and it is the paradox New York City is watching play out in real time with a clarity that should concentrate minds.
According to the city's Comptroller, healthcare and social assistance account for more than 22 percent of New York City employment, but the growth is being driven disproportionately by home health aides and personal assistance workers averaging $31,000 to $37,000 a year, among the lowest average wages of any industry in the city. Consider what that number means against another data point from this winter: when New York Mayor Zohran Mamdani needed bodies to dig out from the Blizzard of 2026, he raised emergency snow shoveler pay to $30 an hour, with overtime pushing toward $45.
More to the point: A home health aide managing a diabetic patient's medication schedule, monitoring vitals, and preventing a hospitalization that would cost the system tens of thousands of dollars earns, on an annualized basis, roughly what the city offered someone to move snow for a few days. The arithmetic is not a policy failure. It is the structural logic of a care economy that has never figured out how to price the work it depends on most.
The Winant pattern is not a Pittsburgh story.
It is the default setting of the post-industrial American city, and New York is running it just as Pittsburgh ran it four decades ago, only with a Medicaid expansion and a Consumer Directed Personal Assistance Program adding bureaucratic infrastructure to what is, at its core, the same biological imperative: a care economy that grows by absorbing social need rather than by generating new economic mass.
Here is what Pittsburgh never had. Here is the distinction that separates The Cardiac Borough thought experiment from the default trajectory.
Pittsburgh was a company town that became a hospital town. It had great research universities — the University of Pittsburgh, Carnegie Mellon — but it did not have the institutional density, the international connectivity, the wealth concentration, or the global reputational authority to position its healthcare economy as an export industry rather than a service economy. UPMC became a regional giant and then a national player and, eventually, an international one, with hospitals in Italy and Ireland and an insurance operation of considerable scale.
But it built that expansion incrementally, reactively, from the inside out. It was not the organizing principle around which the city deliberately constructed a new economic identity. It was the largest thing that happened to survive.
The question that New York must answer, and answer with deliberateness, with the specific quality of institutional will that distinguishes a strategic choice from an evolutionary accident, is whether it can do what Pittsburgh could not: treat the production of cardiometabolic health not as the residue of economic collapse, but as the primary export commodity of a reinvented economy.
Whether it can look at Mount Sinai, NYU Langone, Weill Cornell, Columbia, and NewYork-Presbyterian not as hospitals, but as the clinical engine of a new industrial complex, one in which pharma and care delivery are not separate industries but co-creators, jointly producing a standard of care that is manufactured here, and then refined continuously as a biological process at the intersection of the world's densest drug discovery corridor and its most internationally connected patient base.
And whether it can recognize that a GLP-1 market projected to exceed $250 billion by the early 2030s, plus a $76 billion global medical tourism industry growing at double digits annually, plus an essentially infinite addressable population willing to spend extraordinary sums to remain metabolically healthy, constitute not a clinical problem to be managed, but an industrial opportunity of a scale this city has not seen since finance rewrote the rules of American capitalism in the 1980s.
Pittsburgh's mistake was not that it failed to keep the steel mills open.
The steel mills were going to close regardless, in the way that empires close, not because the will to sustain them was lacking but because the economic physics of the second half of the twentieth century were not compatible with their survival. Pittsburgh's mistake, to the extent that the word "mistake" applies to a city improvising its survival under impossible conditions, was that it received the healthcare economy as a charity rather than seized it as a conquest. The hospitals grew because they had to, not because anyone decided to make them the city's strategic instrument. The same pattern of institutional rigidity that the Burning Man Index measures across industries, the tendency to absorb disruption passively rather than direct it, is what turned a potential conquest into an accident of biology.
There is a version of New York that makes the same mistake. It is not a difficult version to imagine. The version in which the city's extraordinary medical infrastructure continues to expand reactively — more beds for the aging, more Medicaid reimbursements for the poor, more home health aides navigating the outer boroughs on three buses at six in the morning — while the real economic prize migrates elsewhere. Not just the concierge optimization programs serving the global affluent in Dubai and Singapore and Zurich, but the markets that are now visibly forming at the edges of clinical possibility: the cardiometabolic fertility protocols that cross-border patients will soon be traveling to access, as metabolic health and reproductive medicine converge into a single discipline; the early-intervention Alzheimer's programs that affluent families from Seoul to São Paulo are beginning to seek across borders, as lecanemab and donanemab — now approved in more than fifty countries — move from clinical breakthrough to global standard of care; the metabolic risk stratification that a rising global middle class is beginning to understand not as a luxury but as a right.
These markets do not fully exist yet. They are where the evidence is pointing, which is precisely the moment at which a city with the institutional assets to lead them should be making its claim. The production of cardiometabolic health is not a niche for the ultra-wealthy. It is the defining health demand of the twenty-first century, and the city that figures out how to produce it at scale, across income levels and across borders, will have found its next export engine.
New York has not yet decided it wants to be that city.
The Pittsburgh lesson is not that healthcare can replace finance. It may not be able to, and the attempt to force the comparison is probably a category error, since finance in New York operates at a level of abstraction and leverage that no service industry, however sophisticated, can fully replicate.
The difference between a city that becomes its new industry and a city that merely employs it is entirely a matter of whether anyone in a position of institutional power decides to be aggressive rather than passive. UPMC did not save Pittsburgh because the steel industry closed. UPMC saved Pittsburgh because a small number of people within the University of Pittsburgh's hospital system, in the late 1980s and early 1990s, made a series of deliberate strategic decisions to grow internationally, to consolidate aggressively, and to position the institution as a global medical exporter rather than a regional provider.
The cardiometabolic opportunity requires the same quality of decision-making, operating at a higher level of ambition, in a city with incomparably greater assets to deploy.
New York's Cardiometabolic Inflection Point
New York in 2026 sits at an inflection point that Pittsburgh sat at in 1985, with one crucial difference. Pittsburgh's inflection point arrived after the collapse, when the only question was what would fill the void. New York's inflection point arrives before finance has fully surrendered its hegemony, when there is still the institutional bandwidth and the accumulated wealth and the political capacity to make a proactive choice rather than a reactive accommodation.
The question is whether the city's leadership — in medicine, in government, in private capital, in business — has the vision to see what Pittsburgh did not see until after it had no other option.
The terms of that conquest are not complicated.
New York already has the assets. What it does not yet have is a single institution willing to declare, publicly and with full institutional commitment, that cardiometabolic optimization is not a service line but a global export product, and to organize its clinical protocols, its research agenda, its international patient infrastructure, and its pharmaceutical partnerships around that declaration. One Mount Sinai. One NYU Langone. One decision by one health system president to stop thinking like a hospital and start thinking like an export manufacturer.
That is the scale of the intervention required.
Not a policy. Not a public-private partnership convened by the mayor's office and staffed by consultants and public relations teams writing white papers. A decision. Made by one person, in one room, with the specific quality of will that distinguishes intention from an accident. The strategic work required — ecosystem strategy for health systems — is already well-defined. What's missing is the institutional will to commission it.
The Cardiac Borough is not a metaphor for decline. It is a different premise for competition.
/ jgs
John G. Singer is the founder and Executive Director of Blue Spoon and the author of When Burning Man Comes to Washington: A Field Manual for Riding Chaos. Hardcore Zen is published weekly on Substack.