
The Cardiac Borough, Part II — Not One New York Hospital Makes the Cut

The Cardiac Borough is a four-part strategic essay series examining whether the production of cardiometabolic health can replace the gravitational economic role Wall Street has played in New York for a century. Published by Blue Spoon, the series applies ecosystem-centered market strategy — the idea that industries organize around production systems, not products — to the question of what happens when healthcare becomes a city's dominant export. Part I is here.
Part II runs longer than Part I. The argument required it. If you want to start somewhere specific, the section called "The City That Sleeps" is where New York's healthcare infrastructure gets its verdict.
BlackRock chief executive Larry Fink went to Washington this month and said the word "crisis" in public, which for a man whose net worth depends on the precise calibration of his alarm, is the equivalent of a fire marshal pulling the alarm himself. The occasion was BlackRock's infrastructure summit. The crisis, as Fink named it, was labor.
Artificial intelligence is going to create enormous numbers of jobs, he told the room, and society is not prepared to fill them.
This is not the way the AI story is usually told. The dominant narrative is displacement: machines replacing workers, software swallowing occupations, human beings almost incidental, a replay of the automation shocks that hollowed out factory towns in the late twentieth century. In that telling, the future belongs to code and the thinking machines who write it.
Fink's point was the opposite. The constraint, he argued, will not be software.
The real bottleneck is biological. There simply aren't enough people being born, raised, or trained fast enough to translate powerful technology into a working economy. Technical invention is now the easy part. Diffusion is the hard part.
Every technological boom in history has ultimately collided with the same problem: the system that produces workers adapts far more slowly than the technology that creates demand for them. The railroads needed surveyors, bridge engineers, steel workers, and track layers faster than the country could train them. The electrification boom of the early twentieth century required armies of linemen and power engineers that technical schools had barely begun to produce. The interstate highway system turned civil engineering departments into assembly lines for a generation.
The technology arrives suddenly. The workforce arrives late.
AI will follow the same pattern, but in stranger ways. The jobs it creates will not necessarily look like the jobs it replaces. When a new technology spreads, it tends to create entire layers of new work around it: people who translate it, regulate it, audit it, maintain it, explain it, insure it, litigate it, and adapt institutions to it. Entire professions appear not because the technology requires them directly, but because society does.
During its infrastructure summit, New York City-based BlackRock announced a $100 million initiative for trade-work training, a type of investment more commonly associated with hospital systems and insurers that have spent years funding workforce pipelines of their own. The scale is notable, but the signal is clearer: when an asset manager begins funding workforce development, it suggests the constraint has shifted.
The next economy is not waiting on capital. It is waiting on people.
To make his point visceral, Fink brought along Mike Rowe, television's patron saint of manual labor, a man whose entire career is an argument that the country made a category error when it told an entire generation that the only dignified life ran through a four-year degree. Rowe had recently toured a BlackRock-owned data center in Plano, Texas, where electricians are making north of $240,000 a year. Intelligence may be artificial, but the economy around it isn't. The algorithm needs the electrician. The LLM needs the pipe fitter. The server needs the hand.
But training an electrician still takes years. Training a nurse takes years. Training a doctor takes more than a decade. And the companies building the AI economy, the hyperscalers, the financiers, the infrastructure giants, they all know it. Because technological revolutions that grow without workers eventually produce something worse than unemployment. They produce anger. In Washington policy circles there's already a blunt phrase for the outcome: economies that grow without people end with heads on pikes.
AI can generate code in milliseconds. And if Mark Zuckerberg is to be believed, it may soon generate a fountain of medical cures, so many and so fast that the process itself becomes "boring", breakthroughs arriving with the regularity of software updates. This is a remarkable claim from a man who runs a social media company, but set that aside.
The more interesting question is what happens after the cure arrives? Who builds the system that identifies the patient who needs a cure at 4 rather than 74, gets it covered by the health plan, integrates it with the sensor data and the longitudinal record, monitors the response, and adjusts the protocol over the following decade?
Zuckerberg has no answer to this because the question does not arise within the Standard Model. The cure is the easy part. The production system is the hard part. And the hard part is where the durable economic value lives, not in the breakthrough, but in the care and service infrastructure built to diffuse it.
The Real Economic Moat: Longitudinal Metabolic Data
In 1998, Kevin Kelly published New Rules for the New Economy and described the strategic physics of this moment decades before it arrived.
The old economy ran on scarcity, he said: control something rare and the rarity protects you. The new economy will run on abundance and connection. In a network, value accrues not to the node that locks something down but to the node that connects most. The more that join the network, the more valuable membership in it becomes. He called one of his laws the Law of Plentitude. He called another Follow the Free: give away what you can replicate cheaply, because giving it away builds the network, and the network is the asset.
At least 118 companies mentioned their AI "moat" in earnings calls this quarter, a record. The word has become the tic of the anxious executive: a verbal gesture toward the thing that will protect the business when the thing it built can be rebuilt from scratch by a model that costs nothing to run. What Kelly could not have anticipated is what Fink and many others are now describing from different angles: a new economy doesn't really require a Silicon Valley; it requires a different physical + people layer so capital-intensive, so constrained by the laws of materials science and manufacturing, so dependent on the accumulated knowledge of human hands, that it begins to resemble, in its strategic logic, the industrial economy it supposedly superseded.
The software is abundant. The electrician is not.
There is little evidence that investors are buying most of those AI moat narratives. Palantir is doing fine. But Uber CEO Dara Khosrowshahi told Semafor's Compound Interest show last week what the rest of the market is beginning to feel in its bones: "If you're a thin UI layer on top of, let's say, [legacy] systems of record, you're going to have to earn your keep."
He meant it as a warning about software. He was also, without knowing it, writing the investment thesis for the next decade of American healthcare.
The deepest moat in a networked economy is not a patent, not a platform, not twenty years of grinding. It is a body, one specific body, with three years of continuous glucose readings and a longitudinal metabolic record and a drug it has taken every week, a record that is personal and irreplaceable and impossible to replicate by a competitor offering a better technical input today. Multiply that by millions of bodies, each one different, each one generating its own signal, and what you have is not a traditional industry. What is forming is something closer to a unique system of markets: a self-organizing infrastructure that continuously and progressively reads, interprets, interoperates and optimizes personalized metabolic health across an entire life.
Alzheimer's and type 2 diabetes share 395 single nucleotide polymorphisms related to cellular immunity, neuronal plasticity, and cellular signaling. Nearly half of dementia cases may be linked to modifiable risk factors, many of them cardiometabolic. The same 'cardiometabolic health story' is entangled with fertility. Metabolic health influences ovulation, sperm quality, hormone regulation, and pregnancy outcomes; conditions like insulin resistance and obesity are strongly linked to infertility and complications in both men and women.
In other words, metabolism sits upstream of multiple life outcomes: cognitive health at the end of life, reproductive health at the beginning. This is not correlation by confounding. It is shared molecular architecture, the same genetic blueprint building two diseases simultaneously, in the same body, across the same lifespan.
For the worker whose employer provides no meaningful metabolic health coverage does not simply risk a heart attack. They carry a measurably elevated probability of losing their mind.
The evidence linking metabolism, brain health, and aging is advancing quickly, but the care and service infrastructure, and the big system innovation around it, lags decades behind the biology. And it's here when families encounter the real cost of dementia, when they start doing the math. In northern Thailand, around Chiang Mai, a dementia-care ecosystem built from scratch, largely by Swiss and German expats, now operates roughly nineteen facilities serving Western patients at $3,000–$4,000 per month, often with staffing ratios Western systems struggle to match.
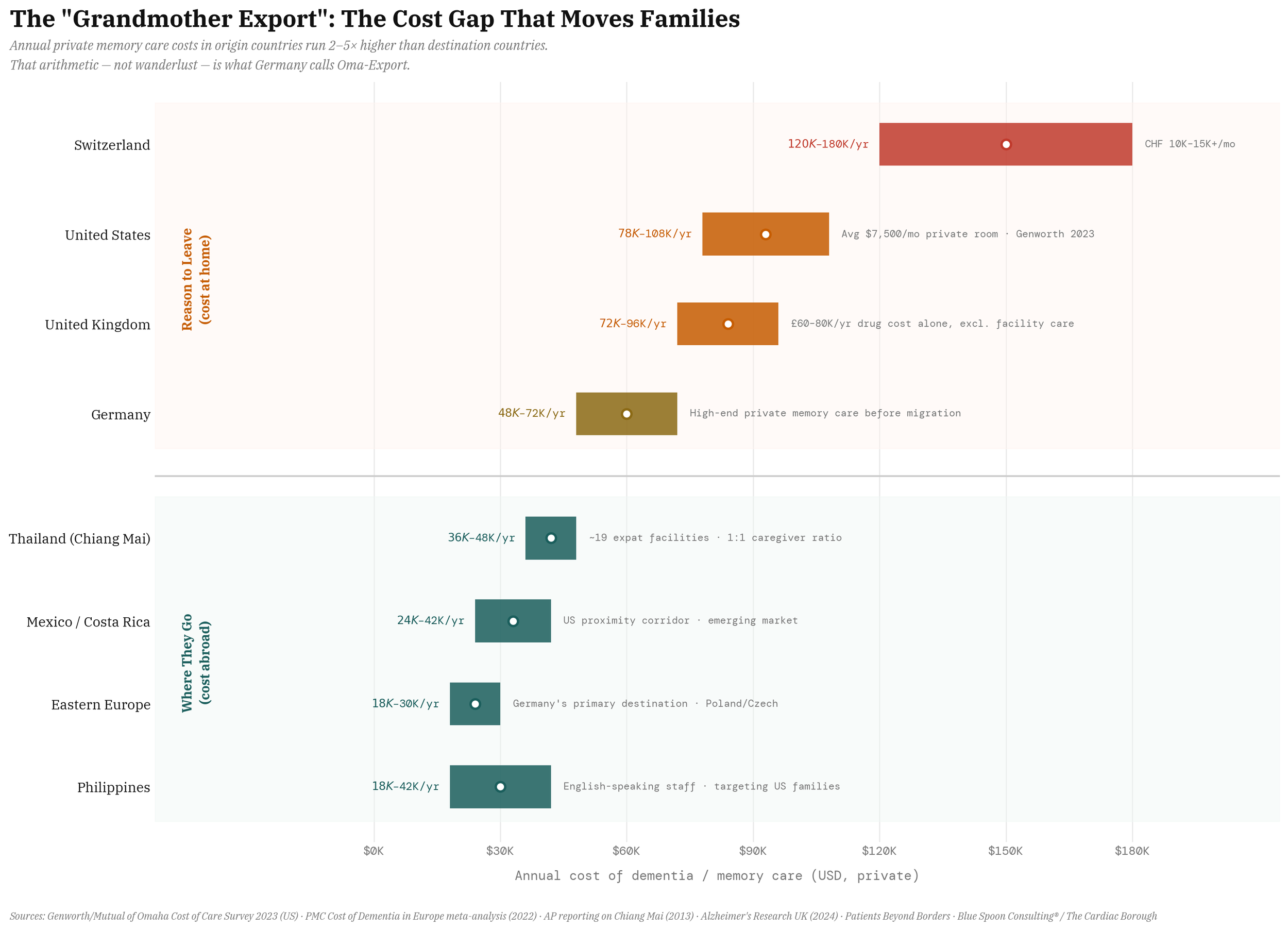
German journalists have given the phenomenon a blunt name: gerontologischer Kolonialismus — gerontological colonialism.
It is not a solution. It is a measurement, the distance between what a healthcare system promises and what it can deliver, denominated in flights to Southeast Asia.
A Framework Built to Miss the Point
On the twelfth of February, 2026, Jake Leach, newly installed as DexCom's chief executive after more than twenty years building the continuous glucose monitoring category from a specialty diabetes device into a $4.6 billion platform business, opened his first earnings call with a sentence that contained, compressed into eleven words, the entire argument the Cardiac Borough is making. "I believe," he said, "we are still early in our journey."
Investors heard a warning about growth.
What Leach was describing was a physical infrastructure in the early stages of becoming something the world has not previously had: a production system for personalized metabolic health at population scale. The investors who sent the stock down are correct that DexCom has not yet built that system. They are incorrect that this constitutes a problem. This is an opportunity so large that the Standard Model cannot see it, not because the evidence is hidden but because the model has no syntax for what the evidence describes. The Standard Model was built to value products. It has spent its entire institutional life building the vocabulary of products, the metrics of products, the religion of products.
The Standard Model understands the world through isolated technical performance and zero-sum competition — products against products, molecules against molecules — and declares the higher efficacy percentage the winner. The logic is linear and narrow in the way that a rifle is linear and narrow: precise within its range, blind to everything outside it.
Five days after DexCom's call, that logic sent Zealand Pharma's shares down more than 30% when their experimental drug posted a weight loss number that was good, but not as good as Eli Lilly's rival in an earlier trial. The molecule that worked was punished for not working harder than a different molecule in a different population.
Three weeks later, Novo Nordisk lost roughly $100 billion in market capitalization in a single session when CagriSema, the drug the market had been calling a Lilly-killer, a combination of semaglutide and an amylin analog that Novo had spent years and tens of millions developing, came in slightly below tirzepatide in a head-to-head trial. Not ineffective. Not dangerous. Not even far behind. Slightly below.
The Standard Model registered this as failure, applied the rifle logic, and fired. The drug that nearly matched the best molecule on the market was treated as a drug that had lost.
The personalized health production system — an induction layer and a maintenance layer, designed to function together, for a population of people that will use them not for the duration of a clinical trial but for the rest of their lives — went unanalyzed. There was no framework in which to ask. But the infrastructure DexCom and others are building points somewhere else entirely. Toward a different economic logic, one centered not on products, but on continuous health engagement with the human body over time, and increasingly with the families that support it.
"The patient" is a legal fiction the system invented to generate a billing code. The family is where the disease actually lives.
The cardiometabolic market, in 2026, is a hive — in Kevin Kelly's sense — that is discovering what it wants. Through out-of-pocket GLP-1 spending that has families restructuring household budgets, through CGM utilization rates above 80% in every covered population, through DexCom's Stelo, with $130 million first-year revenue from people without diabetes who simply want metabolic legibility, the hive is demonstrating that it wants continuous, personalized, real-time production of metabolic self-knowledge.
The Stelo at over-the-counter price points is Follow the Free made physical.
And so, for that matter, is every molecule that goes over the patent cliff, not to mention the price cuts now underway in GLP-1s, each one following a different path to the same destination: the moment when a product's value dissolves into the infrastructure's, when what the product costs/price becomes less important than what the system around it knows. Every Stelo customer is a node in a metabolic sensing network whose value, per Kelly's Law of Plentitude, increases with each new member. Someone who has worn a DexCom sensor for three years has generated a longitudinal metabolic record that constitutes a new 'system of record'.
Think about what that means for a construction worker in the Bronx. The annual physical their union plan covers is not a formality. It is, if acted on correctly, a dementia prevention intervention. The elevated LDL the doctor flags early enough is not lipid management. That is neuroprotection. The cardiometabolic benefits a union negotiates into its contract are not just keeping workers healthy enough to show up. They are keeping workers from losing their minds twenty years after they retire.
It is also exactly the kind of data the AI infrastructure buildout will eventually run out of road without.
The models are voracious and the data centers are going up faster than electricians can wire them, but the data wall is coming, the moment when the synthetic training signal exhausts itself and the models need something the internet cannot provide: continuous, longitudinal, high-frequency biological signal from real human bodies living real metabolic lives. The cardiometabolic record is that signal. It is the feedback loop the AI economy does not yet know it is building toward, the place where the wealth generated by one infrastructure buildout flows into the infrastructure that gives it something true to learn from.
Two capital waves, moving in opposite directions, about to discover they need each other.
Think about what that means for a city that moves before the collision, that spends the years before the two waves converge building the clinical relationships, the sensor networks, the longitudinal records, the manufacturing depth, the contracts that make it the destination rather than the address. A city that does this is not administering a healthcare system. It is not running a social program. It is owning the infrastructure that the AI economy will eventually need to pay to access — the biological signal, the production system, the continuously generated evidence about the human body that no model can synthesize and no competitor can replicate. That city is not looking at a cost center.
It is looking at a royalty stream.
Flying for Fertility
Now consider fertility in the same register, because the population affected is not abstractions in a clinical trial but the children of the workers Larry Fink is trying to train and the families those workers are trying to build.
Polycystic ovary syndrome affects 12% of women globally and is the leading cause of anovulatory infertility. It is simultaneously a cardiometabolic and a reproductive disease, one condition expressing through two organ systems, not two conditions sharing a patient.
The mechanism runs through insulin resistance. A 2024 meta-analysis of 6,137 PCOS women undergoing IVF found insulin resistance associated with lower pregnancy rates, higher miscarriage rates, fewer mature oocytes. The ovary, like the brain, is a target organ for cardiometabolic dysfunction. Leave the metabolism untreated and the embryo count falls, the miscarriage rate rises, and the couple spends another $15,000 to $20,000 on another cycle, money that a firefighter in Staten Island or a teacher in Brooklyn does not have, money that the IVF coverage the building trades and municipal unions have fought for in contract after contract was supposed to prevent the need to find.
A randomized study of obese PCOS women undergoing IVF found liraglutide combined with metformin produced a pregnancy rate per embryo transfer of 85.7% compared to 28.6% for metformin alone, despite comparable weight loss in both groups. The effect was not metabolic. It was reproductive. GLP-1 receptors are expressed in ovarian and endometrial tissue; the drug improves ovulation and implantation through pathways independent of body weight. The question of whether a union health plan covers it is not an actuarial question. It is a question about whether working families get to have the children they are trying to have.
The families running this arithmetic without a benefits package that helps are running it internationally.
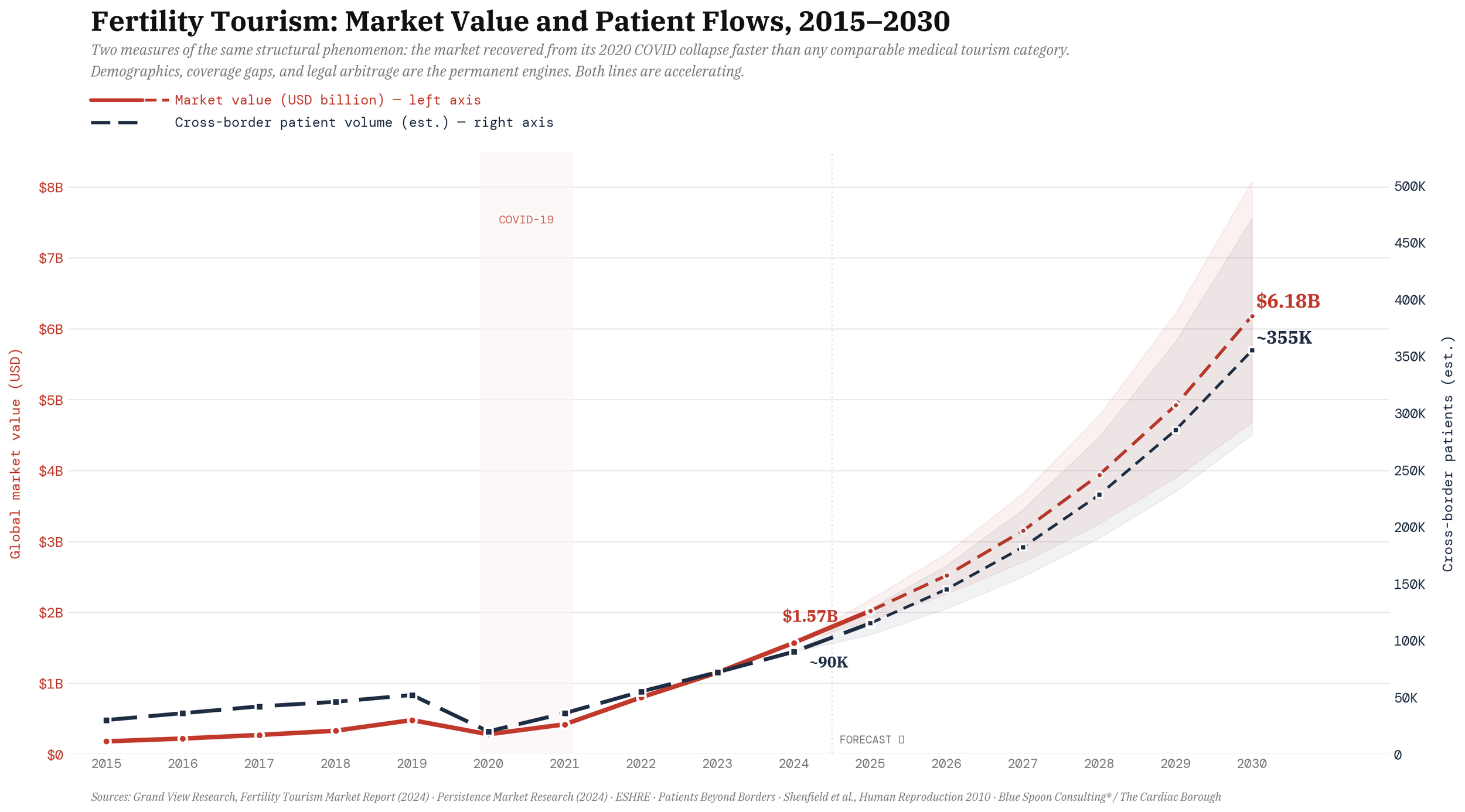
The global fertility tourism market — already at $1.6 billion and growing at roughly 25% annually — is built almost entirely on the gap between what reproductive medicine costs where patients live and what it costs somewhere else. Spain has become the primary destination for European donor-egg IVF; American patients cross to Mexico, Canada, the Czech Republic. The market expands because domestic access remains rationed by price. Ask any reproductive endocrinologist and they will tell you the truth of it: the fertility drugs crossing those borders are rarely some new scientific thunderbolt. They are biosimilars, generics, and near substitutes from the same hormonal playbook, prodding the same pathways and yielding much the same results.
The market is not moving toward better medicine. It is moving toward cheaper access to the same medicine, which is Follow the Free operating at the level of national borders.
And at the scale above the union contract, it is a question about whether the United States and China, two nations watching their birth rates fall and their demographic futures narrow with each passing census, have the wit to understand that the fertility crisis they are spending billions to address with subsidies and tax credits and exhortation is, in measurable biological part, a cardiometabolic crisis. The solution is not a $1500 check written to a young couple in a bid to boost birth rates, but an infrastructure built around the body that is trying to carry the child.
The Standard Model has no category for any of this.
A GLP-1 is a diabetes drug or a weight-loss drug or, tentatively, a cardiovascular drug. The possibility that it is simultaneously a neuroprotective agent, a fertility enhancer, and a cardiometabolic maintenance platform — expressions not of separate applications but of a single underlying mechanism — does not fit the trial architecture or the reimbursement code or the investor model.
The philosopher Michael Sandel has spent his career at Harvard arguing that markets corrupt the goods they are asked to price, that the act of commodifying something changes what it is. His book on the subject, What Money Can't Buy, is the most readable account of why the Standard Model keeps mislabeling the opportunity in front of it. But the demand curves in this market do not need a philosopher to explain them. They are inelastic not because pricing corrupts sacred goods, but because the substitutes are catastrophic.
The CGM consumer is not paying for a sensor. They are paying for metabolic legibility, for the irreversible experience of a body that was opaque becoming readable. The fertility couple is not paying for an IVF cycle. They are paying for a child. The family keeping a parent in Chiang Mai is not paying for dementia care. They are paying for one more year of recognition. These are the most inelastic demand curves in the economy, because the alternative is not a competitor product. It is the loss of something irreplaceable.
Which returns us to the employer/union health plan.
The plan that covers the annual physical but not the CGM. That covers emergency cardiac surgery but not the GLP-1 that would have prevented it. That covers IVF cycles but not the metabolic workup that would have determined why they keep failing. These are not coverage gaps in the actuarial sense. They are the structural consequence of a system designed around episodes and diagnostic codes when the "unmet need" is a continuous production system whose most valuable intervention points are upstream of every episode it is currently paying for.
The union that negotiates cardiometabolic infrastructure into its benefits package is not spending more on healthcare. It is buying the production system that prevents the expenditures the Standard Model is currently forced to cover.
What a BlackRock and a Mount Sinai and a DexCom and a Zealand can build together is not a service line. A service line is what a hospital system creates when it wants to extract more revenue from a diagnosis it already owns.
What these four entities can build, if they understand what they are sitting on, is a new premise for how the cardiometabolic economy organizes itself: around the recognition that metabolic disease, cognitive decline, infertility, and the slow biological unraveling that the Standard Model treats as separate specialties are in fact one condition, moving through one bloodline, across one lifetime, managed not by the patient who receives the diagnosis but by the household that absorbs it. The mother who monitors her glucose. The father whose sperm count is falling with his testosterone. The grandmother in Chiang Mai whose LDL nobody treated at 44. The daughter who will pay, one way or another, for all three.
The City That Sleeps
Last month Mayor Zohran Mamdani traveled to Washington and asked Donald Trump for $21 billion to deck over Sunnyside Yard: 12,000 new affordable homes, 30,000 union jobs, the largest housing investment New York City has seen in fifty years.
Three days earlier, the city's Department of Investigation found the New York City Housing Authority had allowed its vacant apartments to more than double, from 2,800 to 6,700 — while 165,000 families wait, 600 units sit squatted, the average turnaround runs 326 days, and the capital repair gap stands at $80 billion. The juxtaposition is diagnostic. The city cannot maintain the infrastructure it already owns and its mayor is proposing to build more.

This is what public infrastructure does in its later decades: it becomes a monument to the ambition that built it and a rebuke to the will that was supposed to sustain it. The city's healthcare infrastructure tells the same story from a different angle, and the angle is worse.
When Walmart needed complex surgery for 1.1 million employees in its health plan, it built its own network of centers of excellence — Mayo Clinic in Rochester, Minnesota, Cleveland Clinic in Cleveland, Geisinger in Danville, Pennsylvania, Virginia Mason in Seattle, Mercy in Springfield, Missouri — covering the procedure in full, travel and lodging for patient and companion included. When Boeing needed cardiac care for 83,000 employees and retirees, it contracted directly with Cleveland Clinic, fixed price, full travel included. When Lowe's needed spine and cardiac surgery for its workforce, it went to Cleveland Clinic. When PepsiCo needed spine surgery, it went to Johns Hopkins in Baltimore. General Electric followed the same logic.
The pattern, established over more than a decade of direct employer contracting, runs through Rochester and Cleveland and Danville and Seattle and Baltimore….through every region of the country, to systems selected not for their famous names but for their outcomes data, their economic innovation, and their operational capacity to receive workers flying in from across the country and send them home with a guaranteed result.
Not one New York City hospital system appears on any of these lists.
Fifteen major hospital systems. The largest concentration of clinical researchers on the eastern seaboard. A pharmaceutical corridor from Midtown through the Hudson Valley. Memorial Sloan Kettering, NYU Langone, NewYork-Presbyterian, Mount Sinai — institutions the city spent generations building and that the country regards as among its finest. And when American employers designed the clinical infrastructure that would determine where their workers received the most complex and consequential care of their lives, they looked past New York entirely.
New York has the prestige. It does not have the contracts. That is what it means to have a density without an ecosystem strategy. The assets exist. The 'production of health system' does not.
And a city that cannot convert its clinical density into the contracts and outcomes infrastructure that make it the destination for workers, for employers, for the cardiometabolic economy that is now assembling itself around exactly the kind of longitudinal, integrated, continuously produced health that New York's institutions are, in theory, positioned to provide, is a city that is building NYCHA again. Larger. More expensive. Announced at a press conference. Unmaintained by the thirty-fifth year.
The Density Exists. The Strategy Doesn't.
The infrastructure being assembled in the cardiometabolic market is built from continuous data flows, clinical relationships, manufacturing ecosystems, and the accumulated metabolic records of millions of patients who have decided, without being asked by any government, that continuous personalized health production is worth paying for — workers included, workers especially, in their out of pocket spending on Ozempic and CGMs and fertility treatments their benefits packages don't yet cover.
This is not a market waiting to be created. It is a market already voting, with its own money, against an economic system that has failed to meet it.
That system — organized to serve and sustain the administrative machinery of claims adjudication, prior authorization, and contract disputes — is revealing its own obsolescence in real time. In New York, right now, Mount Sinai and Anthem are locked in the kind of negotiation failure that throws thousands of patients out of network and reminds everyone involved that the existing infrastructure was built to adjudicate episodes, not produce health. The contracts exist to manage the cost of what went wrong. They have no architecture for the continuous management of what could go right. Capital that remains attached to that machinery — to the billing cycle, the authorization queue, the renegotiation every three years — is capital that has chosen the thirty-fifth year of NYCHA over the production system that doesn't need a federal monitor to function.
Instead, BlackRock-level capital could begin attaching itself to something else: the continuous management of health and the continuous production of evidence about the human body. Not the episode. The life. Not the claim. The record.
In a world where software is abundant and free, the place that builds the hardware wins. New York City has the density, the hospital systems, the researchers, the pharmaceutical corridor, the union workforce whose collectively bargained plans represent one of the largest pools of organized healthcare purchasing power in the country.
What it does not have is an ecosystem strategy, one that converts that density into the contracts, the production systems, the longitudinal infrastructure, and the clinical relationships that make it the destination rather than the address.
The union member paying out of pocket for the cardiometabolic infrastructure her health plan doesn't cover is not a coverage problem. She is a market signal, the clearest one available, denominated in her own money, pointing toward the infrastructure that does not yet exist and the city that could build it. The gap between what she needs and what the plan provides is not a failure of coverage. It is an invitation.
And markets, unlike concrete, belong to whoever is first to understand what they are building — and why it holds.
/ jgs
John G. Singer is the founder and Executive Director of Blue Spoon and the author of When Burning Man Comes to Washington: A Field Manual for Riding Chaos. Hardcore Zen is published weekly on Substack.