
The Cardiac Borough, Part III -- The Enrollment is the Platform

The Cardiac Borough is a four-part strategic essay series examining whether the production of cardiometabolic health can replace the gravitational economic role Wall Street has played in New York for a century. Published by Blue Spoon, the series applies ecosystem-centered market strategy — the idea that industries organize around production systems, not products — to the question of what happens when healthcare becomes a city's dominant export. Part I is here. Part II is here.
Part III is the longest in the series. It is also where the argument stops being about what New York has and starts being about how New York can build. The section called "Assembly Rules" is where the union network argument begins and where the logic of the series snaps into place. The section called "What Kai-Fu Lee Missed" is where the biological data competition gets its fullest treatment. If you want the single sharpest entry point, start with "Displacement, Not Decline" and read forward.
There is a word that gets used so often in discussions of urban economic strategy that it has been hollowed out almost entirely: ecosystem.
Every city now claims to have one. Every economic development authority publishes plans to build one. Every mayor announces the initiative that will seed it, names the anchor institution that will anchor it, schedules the ribbon-cutting that will inaugurate it. The word has become the lingua franca of the urban aspiration class — the consultants and the conference organizers and the deputy mayors for innovation who fill the ballrooms of smart city summits, twenty-five thousand of them at a time, to discuss ecosystem integration and AIoT and sustainable inclusive urban development, which is to say, to discuss nothing, in the precise and costly way that people discuss nothing when they have confused the vocabulary of transformation with the thing itself.
The word has traveled so far from its biological origin, the original meaning that Gregory Bateson and James Moore and Stuart Kauffman would recognize, of a system of mutually catalyzing components that becomes self-sustaining precisely because no single node controls it, that it now functions as a kind of organizational poetry: evocative, prestigious, and almost entirely empty of operational content. It describes a destination without a map.
Gregory Bateson, the anthropologist and systems thinker who spent his career mapping the patterns that connect living systems, understood an ecosystem as a system in which the components do not merely coexist but constitute each other, in which the behavior of each element shapes and is shaped by every other.
James Moore brought that logic into business strategy in the 1990s, arguing in The Death of Competition that separate industries were giving way to business ecosystems, communities of markets and organizations that co-evolve and share capabilities around a strategic direction, in which no single firm controls the whole but every firm depends on the health of the whole. Stuart Kauffman, working from the mathematics of complexity, named the threshold condition: the autocatalytic set, the point at which the components of a system become mutually enabling, each one catalyzing the reactions that sustain the others, the system crossing from fragile assembly into self-sustaining life.
Bateson mapped the pattern. Moore applied it to markets. Kauffman gave it a mechanism. All three were describing the same thing: a system that, once it achieves sufficient density of mutual catalysis, does not need to be managed into existence. It summons itself.
What is discussed at smart city summits is not this. The agenda is operational: how to deploy a sensor network, how to manage a vendor, how to measure a pilot, how to procure AI for grid resilience. Six hundred speakers and eight hundred fifty cities convening in Barcelona to discuss implementation. The question of which production system a city should be building — which flows to position itself at the center of, which assets to convert into platforms that set terms rather than follow them — does not appear on the agenda.
Technology without strategy is not an ecosystem. It is inventory.
What Pittsburgh actually built — not planned, not announced, but built, metabolically, over forty years of the painful and unintentional adaptation this series began with — was the real thing. The University of Pittsburgh Medical Center (UPMC) did not appear because someone decided Pittsburgh needed a healthcare ecosystem. It appeared because steelworkers aged and got sick and needed care, and the wives and daughters who had been pushed to the economic margins of the mill economy entered the healthcare workforce to replace the income the mills had stopped providing, and Medicare and Medicaid created the insured patient base that made the care economy financially viable, and a medical school that had been training doctors since 1886 found itself, almost accidentally, at the center of an economic transformation it had not engineered and barely understood while it was happening.
The ecosystem was not designed. It was summoned.
New York is not Pittsburgh. It does not have the luxury of waiting forty years for the metabolic response. It has the institutions, the capital, the patient base, the research infrastructure, and the union workforce already assembled. What it lacks, what Parts I and II of this series have been building toward, is the strategic framework that converts density into production, assets into systems, and the largest concentration of healthcare resources on the eastern seaboard into the thing that DexCom's Jake Leach described on his February earnings call: something the world has not previously had.
The question Part III is trying to answer is simpler and harder than it sounds.
What does it actually mean for a city to become a platform for the production of cardiometabolic health? Not a hub. Not a cluster. Not an ecosystem in the hollow meaning of that word. A platform in the biological definition, one that describes a better economic system whose participants build on top of it, whose business and market value increases with every node that joins, and whose infrastructure becomes more irreplaceable the more deeply it is embedded in the lives of the people who use it.
The answer begins with a fact that the smart city summits rarely pause on: the city is winning. Not in the political register, not in the quality-of-life debate that oscillates between urban revival and suburban flight, but in the demographic reality that admits no serious argument. In 1950, one person in five lived in a city. Today, nearly three in five do. By 2050, two in three will. The number of megacities — urban areas of ten million or more — has quadrupled since 1975, from eight to thirty-three, and the UN projects seven more by midcentury. The total number of cities on earth has doubled since 1975. Two thirds of all population growth between now and 2050 will occur in cities.
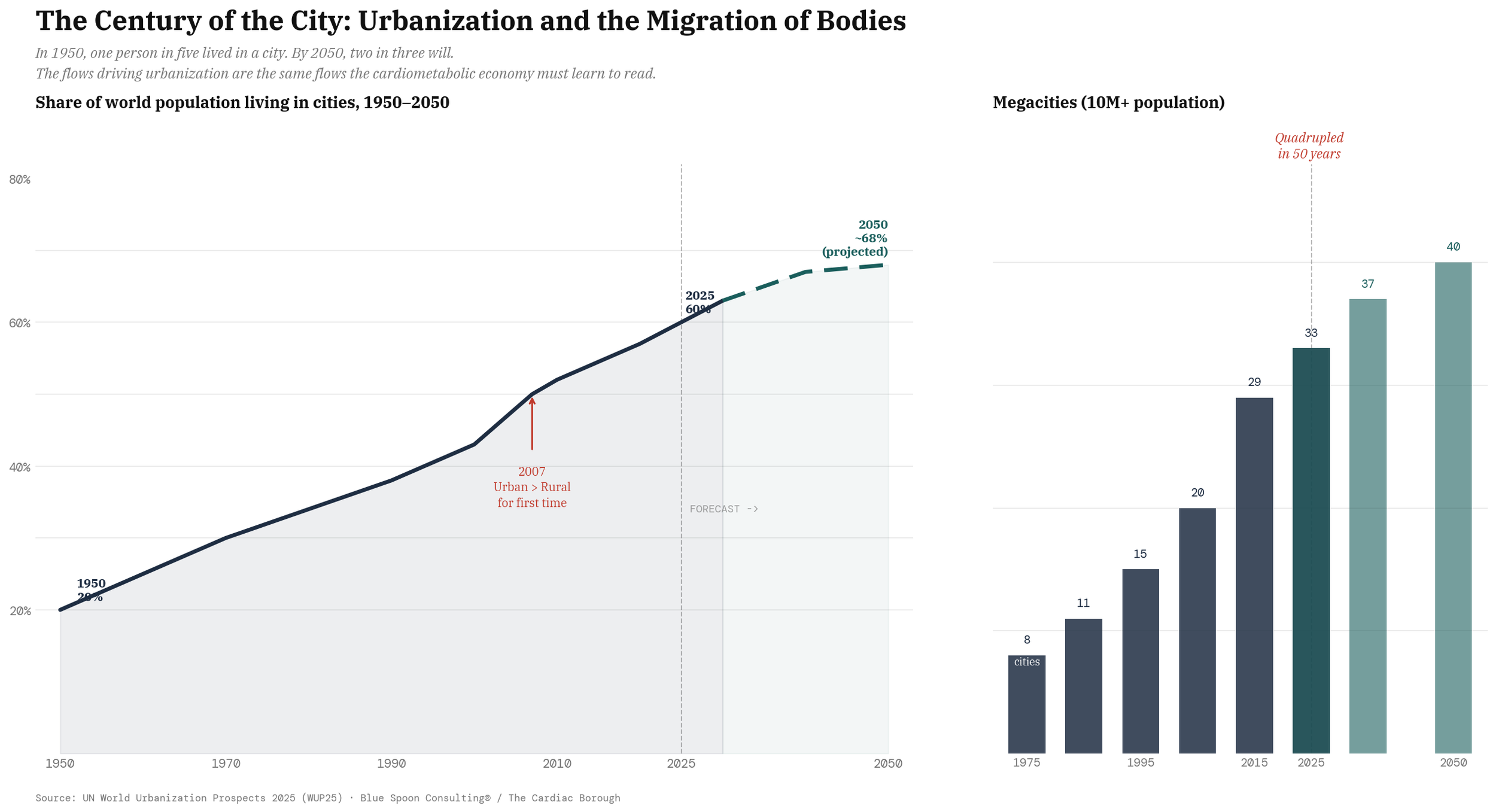
This is not an urban planning statistic. It is a cardiometabolic one.
Every person who moves from a rural area to a city undergoes a metabolic transition, a shift in diet, activity pattern, stress load, sleep architecture, and exposure to environmental risk factors that is among the most powerful drivers of cardiometabolic disease in the epidemiological literature. Urbanization is the largest uncontrolled metabolic experiment in human history, running continuously, on billions of subjects, without a protocol or a principal investigator. The city that builds the infrastructure to read that experiment — to monitor, interpret, and act on the continuous biological signal generated by its population — is not just building a healthcare system.
It is building the most valuable data asset in the world.
Displacement, Not Decline
Manuel Castells, the Spanish sociologist whose three-volume The Rise of the Network Society became the most cited work in urban studies of the late twentieth century, spent the 1990s trying to describe what was happening to cities in the network economy, and his central finding was that the informational economy does not make geography irrelevant. It makes it more selective. In his formulation, "functionality, wealth, and power are defined in terms of flows."
In the industrial economy, proximity to raw materials or manufacturing capacity determined which cities grew. In the network economy, Castells argued, what determines which cities grow is their position in the global flows of capital, information, and talent — whether they are nodes through which value flows, or nodes that value flows around. "Any node that disconnects itself is simply bypassed." The cities that became global in the network economy — New York, London, Tokyo, later Shanghai and Shenzhen — did not win because they were largest. They won because they were most connected to the flows that mattered, and because the institutions concentrated in them made those flows legible, trustworthy, and valuable in ways that no other geography could replicate.
A platform is not a place.
It is not a building or a district or an incentive package. It is not a technology. It is what Castells was describing: a node in a network so deeply embedded in the flows that matter that its removal would cost the network more than any other node's removal. The App Store is a platform. The interstate highway system is a platform. The New York Stock Exchange, at its peak, was a platform — the rules, the relationships, the physical and informational infrastructure that made it easier and cheaper and more credible to raise capital in lower Manhattan than anywhere else on Earth, and that attracted the talent and the institutional density that made that advantage self-reinforcing for a century.
What made Wall Street a platform was not the buildings. It was the system of trust, liquidity, information flow, and institutional relationships that made a share of stock issued in New York worth more, and more readily tradeable, than one issued anywhere else. The platform produced a premium. The premium attracted participants. The participants deepened the platform. The cycle was autocatalytic in exactly the sense Kauffman describes: mutually enabling components, each one catalyzing the others, the system becoming more valuable and more durable with each new participant.
Wall Street's platform premium is eroding.
Trading has been commoditized by electronic markets. The information advantages that required physical proximity have been dissolved by technology. The talent that once had no choice but to be in lower Manhattan now has choices, and many of them are exercising those choices. The platform is not dying — it is too deeply embedded in the legal, regulatory, and institutional infrastructure of American finance to collapse quickly — but its gravitational pull is weaker than it was, and the next generation of participants is not organizing its economic life around it with the same inevitability their predecessors did.
In Castells' framework, what is happening to Wall Street is not decline. It is displacement. The flows that once had no choice but to route through lower Manhattan are finding new paths, new nodes, new geographies that are more embedded in the flows that now matter. The question for New York is not how to slow that displacement. It is which new flows to position itself at the center of.
This is the opening.
Not the opportunity to replace Wall Street with something that looks like Wall Street, a new financial center, a new trading floor, a new concentration of capital-allocating institutions. Not the campaign to make the city affordable by managing its decline. The opportunity is to build a platform whose premium derives from something Wall Street's platform never had: the human body itself, and the continuous, irreplaceable, longitudinally deepening record the body generates when the right infrastructure is built around it.
The city that builds this platform is not administering a public health system. It is creating the conditions under which fifteen million inhabitants become, in the most literal economic sense, stakeholders in the infrastructure their bodies are generating — not the passive subjects of a care system that extracts value from their disease, but the nodes of a network whose appreciation they share in, the real fortune at the bottom of the pyramid sitting not in cheap labor or subsidized consumption but in the longitudinal biological signal that no other asset class can replicate and no competitor geography can steal.
The cardiometabolic platform premium would work the same way Wall Street's did, but with a different asset at its center.
Instead of liquidity and information about capital, the asset is longitudinal biological signal and the unique combination of business relationships that make that signal legible, actionable, and continuously improving. Instead of the trust premium that made a New York listing worth more than a listing elsewhere, the platform premium would be the clinical depth premium, the accumulated evidence, the protocol density, the sensor network scale, the research relationships that makes a cardiometabolic intervention delivered through the New York platform worth more, and more likely to produce the outcome the patient is paying for, than one delivered anywhere else.
What Kai-Fu Lee Missed
Kai-Fu Lee, the former Google China president who became one of the most precise analysts of the AI competition between the United States and China, argues in AI Superpowers that the decisive advantage in the AI era will not belong to the country with the best algorithms. Algorithms, he says, are increasingly commoditized: the research is published, the architectures are shared, the techniques diffuse. "Beyond that point, data makes all the difference."
As Lee puts it, "algorithms tuned by an average engineer can outperform those built by the world's leading experts" if they are trained on far more data. The decisive advantage, in other words, will belong to the country with the best data — the richest, most diverse, most longitudinal data, the kind that can only be generated by a population living its actual life, making actual decisions, producing actual biological and behavioral signal at scale, continuously, over years.
For Lee, China's advantage is not just that it has more internet users. It is that Chinese platforms capture a denser merger of online and offline life: payments, food delivery, ride-hailing, and other everyday transactions all flow through the same digital systems, producing behavioral data from the physical economy, not just the web. The United States, by contrast, remains stronger in frontier research but more constrained to internet-native data domains, with weaker access to the full stack of everyday transactional life.
Lee wrote AI Superpowers in 2018, before the GLP-1 revolution, before the CGM entered mass consumer markets, before the cardiometabolic record emerged as a distinct category of biological signal with properties that behavioral data cannot replicate. He was describing the competition for consumer behavioral data — clicks, purchases, navigation patterns, social interactions. The competition he did not describe, because it had not yet become visible, is the one for continuous longitudinal biological data, the kind generated by a body wearing a sensor every day for three years, taking a drug every week, tracking its metabolic response to food and exercise and sleep and stress in real time.
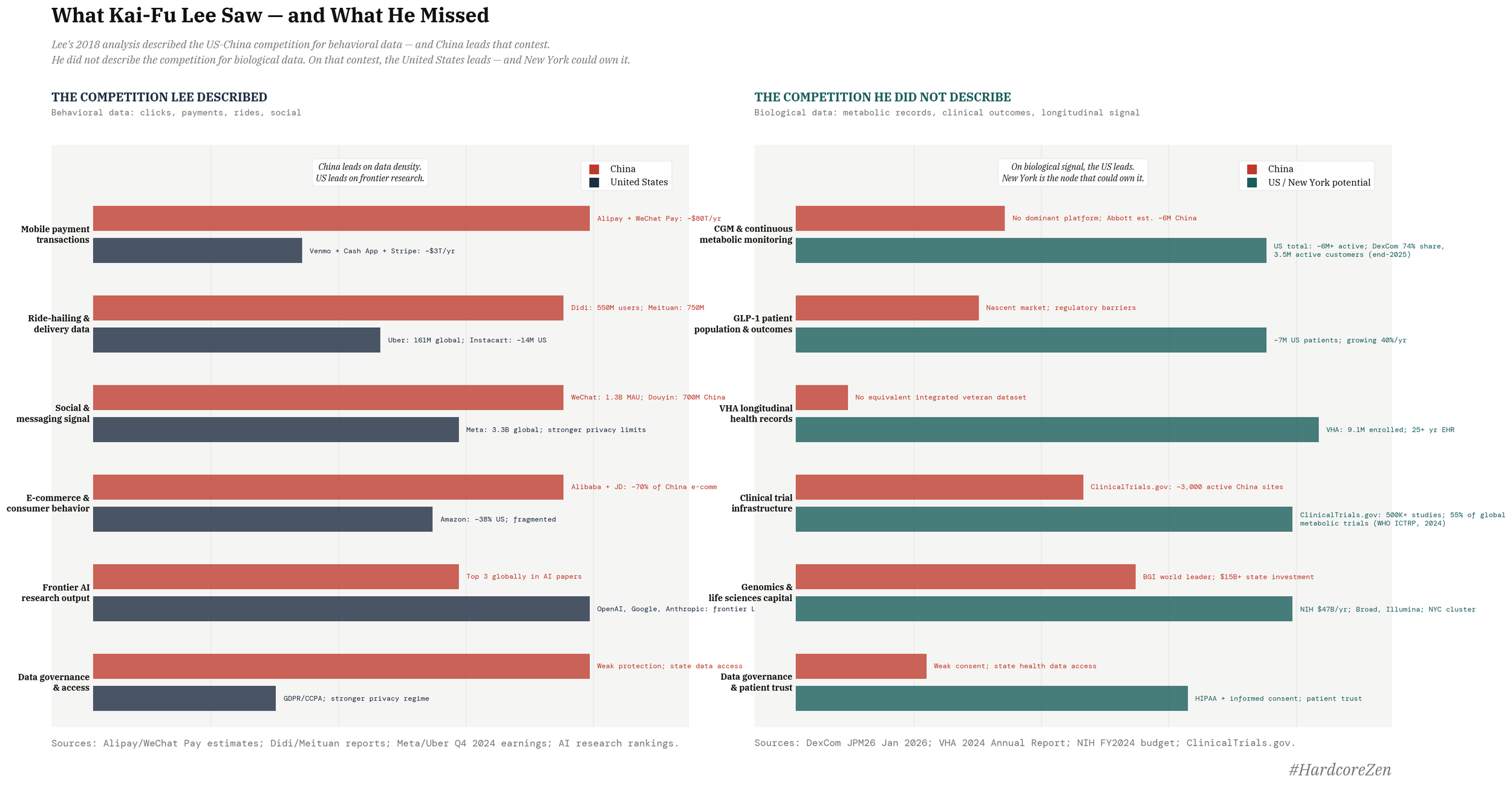
This data is not behavioral. It is biological. It cannot be synthesized. It cannot be generated by a model trained on historical records.
It must be produced by real bodies, in real time, in a real production system. And the geography that builds the deepest production system for it — the most enrolled population, the most sophisticated clinical protocols, the most developed research infrastructure, the most trusted institutional relationships — will own the data advantage that Lee was describing, applied to the most consequential domain of human biology.
How The Platform Gets Built
A cardiometabolic platform for New York is not a single institution or a single initiative. It is three layers, each one building on the one below it, each one catalyzing the others.
The first layer is the physical infrastructure of continuous metabolic monitoring, the sensors, the devices, the manufacturing and distribution ecosystems that put the continuous glucose monitor on the wrist of the construction worker in the Bronx and the warehouse sorter in Queens and the home health aide in the South Bronx who is currently earning $40,000 a year managing someone else's chronic condition while her own goes unmonitored. This layer already partially exists. DexCom's Stelo at over-the-counter price points is the beginning of it. The GLP-1 price cuts that are dissolving the cost barrier to metabolic medication are deepening it.
What is missing is the deliberate, systematic enrollment of New York's entire population into the metabolic sensing network. The city has 8.3 million people across five boroughs. Roughly 745,000 of them are union members whose collectively bargained health plans represent the most organized pool of healthcare purchasing power in the country. Approximately 200,000 are veterans whose care through the Veterans Health Administration has already generated one of the largest longitudinal health datasets in existence. The roadmap begins with those two populations and extends outward until the city's full population density becomes the asset it has always had the potential to be.
The second layer is the clinical and institutional infrastructure that makes the data from those sensors actionable.
This is where New York's density is most obviously an asset and most obviously underutilized. Memorial Sloan Kettering, NYU Langone, NewYork-Presbyterian, Mount Sinai — these institutions have the clinical depth, the research capacity, and the patient relationships to build the protocols, the outcome standards, and the evidence base that would make New York the destination for complex cardiometabolic care the way Cleveland Clinic is the destination for cardiac surgery. The center-of-excellence map from Part II tells the story in reverse: the absence of New York from the lists of employers' preferred clinical partners is not a verdict on the quality of New York medicine. It is a verdict on New York medicine's failure to organize itself as a production system, to build the bundled pricing, the outcomes guarantees, the care coordination infrastructure, the medical tourism and the employer relationships that convert clinical excellence into a platform others want to build on.
The third layer is the data and research infrastructure that converts the metabolic records generated by the first layer and the clinical outcomes produced by the second layer into something that has never previously existed at scale: a longitudinal biological system of record for an entire urban population, continuous, irreplaceable, and deepening with every sensor reading and every clinical encounter and every year that passes without a competitor geography having built the same thing.
This is the layer that turns the platform from a healthcare system into a royalty stream. Not the kind of royalty stream that accrues to a patent or a social media network that captures attention and sells it to advertisers; those are businesses, and large ones, but they are built on signals that can be replicated, on behavior that can be modeled, on attention that will eventually migrate to the next interface. The biological record cannot migrate. It cannot be replicated. It accumulates in one direction only, across one lifetime, in one body, and the infrastructure that holds it becomes more valuable with every passing year in a way that no software and no advertising network and no large language model trained on the text of the internet can match. Because what it holds is not a representation of life but life itself, denominated in glucose readings and metabolic trajectories and fertility outcomes and the slow molecular architecture of a population that chose, or was given the infrastructure, to know itself.
Mark Zuckerberg's empire is built on what people say about their lives. This is built on what their bodies actually do. The difference in durable economic value, measured across a generation, is not small.
Assembly Rules
Platforms are not built all at once. They are built in sequence, and the sequence matters more than almost any other strategic decision. The wrong sequence — building the data layer before the monitoring infrastructure, building the research layer before the clinical protocols, building the commercial relationships before the patient base — produces an expensive institutional structure with nothing to build on.
The right sequence for the New York cardiometabolic platform begins with the union health plans. Not because unions are the most glamorous entry point, but because they are the most strategically positioned one.
The collectively bargained health plans of the building trades, the transit workers, the teachers, the healthcare workers, and the municipal employees represent the single largest organized pool of healthcare purchasing power in the city. And those members are already voting for the platform with their own money, in their out-of-pocket spending on Ozempic and CGMs and fertility treatments their plans don't yet cover. The demand exists. The institutional structure to act on it exists. What is missing is the strategic decision to treat that demand not as a cost to be managed but as the enrollment engine for the first layer of the platform.
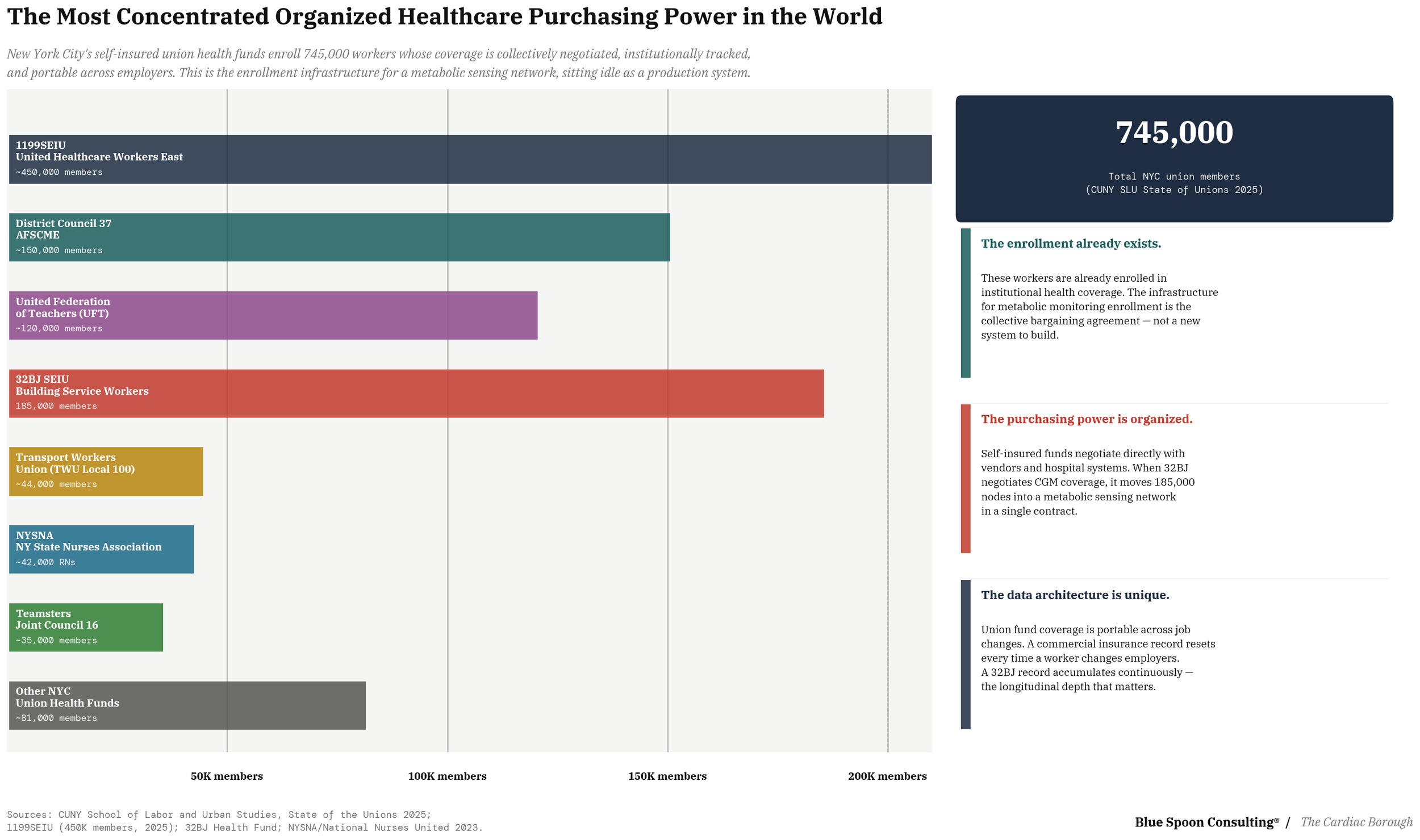
When 32BJ SEIU, the union representing 185,000 building service workers whose Health Fund self-insures across 5,000 New York employers, from small businesses to global real estate firms, negotiates CGM coverage into its benefits package, it is not merely improving health outcomes for its members. It is enrolling 185,000 nodes into a metabolic sensing network and generating the longitudinal biological signal that the second and third layers of the platform require. The 32BJ Health Fund is structurally unusual in American labor: members carry their coverage across job changes without interruption, which means the metabolic record accumulates continuously rather than resetting every time a doorman moves buildings or a cleaner changes contractors.
That continuity is not a benefits design detail. It is the data architecture condition on which the platform depends.
When the municipal unions negotiate GLP-1 coverage that includes the metabolic workup and the continuous monitoring that makes the drug clinically effective rather than episodically prescribed, they are not just buying a drug. They are building the clinical protocol infrastructure that the COE model requires. The sequence runs from union benefits through clinical protocols through outcomes data through employer COE contracts through research partnerships through data licensing — each layer earning the right to build the next one.
The enrollment is not a precondition for the platform. The enrollment is the platform, in its first form, before the city knows it is building one.
Now extend the logic outward, and when you do, understand that what you are looking at is not an incremental improvement in benefits design but a strategic rotation of historic proportions for the medical device and pharmaceutical industries, the kind that happens once in a generation if the participants are paying attention and once in a century if they are not, the kind that does not announce itself as a revolution because it arrives wearing the unremarkable clothing of a contract negotiation.
It is a roadmap drawn in the language of labor relations for displacing Big PBM and the commercial insurers via a worldwide direct-to-employer channel that neither the pharmacy benefit managers nor the carriers saw coming.
They were watching the hospital systems and the health plans and the regulatory agencies, watching all the places power has always lived. The actual disruption was assembling itself one collectively bargained benefits package at a time, in the offices of union health funds that nobody on Wall Street covers and nobody in pharma strategy tracks and nobody in Washington thinks about, until the moment they cannot be ignored.
There are 14.7 million union members in the United States. The European Trade Union Confederation represents 45 million workers across 42 countries. India's largest union federation, the Indian National Trade Union Congress, claims more than 30 million members — and India, whose 1.4 billion population carries the world's largest burden of type 2 diabetes, has twelve recognized national union federations with a combined membership that dwarfs any comparable structure in the developed world. India also, as of last weekend, has generic semaglutide. Novo Nordisk's patent protection expired across countries representing forty percent of the world's population on the same morning that dozens of Indian manufacturers began racing to put a $15-a-month version of the drug that is rewiring the practice of Western medicine into the hands of a population that cannot afford US pricing models.
These are not small numbers. They are the largest organized populations of longitudinal benefit enrollees on the planet, people whose health coverage is collectively negotiated, continuously maintained, and institutionally tracked across years of employment in ways that fragmented individual commercial insurance never does.
And the number is growing.
Public support for unions reached 68 percent in 2025, near levels not seen since the 1960s. Since 2021, petitions for union elections at the National Labor Relations Board have more than doubled, and, according to the Economic Policy Institute, workers are winning their elections in unprecedented numbers. The private sector gained 261,000 new union members in 2023, the first significant increase in decades, driven by healthcare, tech, and logistics. Healthcare workers are unionizing at historic rates. The workforce that will build the next generation of physical infrastructure — the electricians, ironworkers, plumbers, pipefitters, and HVAC technicians that every data center, every energy transition project, every AI facility requires — is overwhelmingly unionized already, and the pipeline is expanding.
This is where the BlackRock story from Part II closes its own loop.
BlackRock projects that employment in infrastructure-related skilled trades will grow by more than 5 percent between 2024 and 2034, considerably faster than the 3 percent national average, translating to hundreds of thousands of net new jobs. On March 11, 2026, eight days before this essay went to press, BlackRock announced a $100 million initiative to train up to 50,000 skilled craft workers, with the National Association of Building Trades Unions announcing simultaneously a new agreement with OpenAI to link its 14 craft unions to growing sector demand for data center infrastructure. The people who will build the physical substrate of the artificial intelligence economy are union members. They will be covered by union health funds. Those health funds will negotiate their benefits.
The question is whether anyone thinks to negotiate metabolic monitoring into those benefits, and to understand what gets built when they do.
Every collectively bargained benefits package that includes CGM coverage, GLP-1 protocols, and outcomes tracking is a data production agreement dressed in the language of labor relations. This is where the market access argument for pharma inverts entirely. The conventional market access problem is reimbursement: getting payers to cover a drug once it is approved.
The emerging problem is something harder: demonstrating real-world clinical effectiveness across diverse populations, generating the outcomes data that regulators in the EU, Japan, and the United Kingdom are increasingly demanding as a condition of sustained coverage, and doing it at a scale and longitudinal depth that randomized controlled trials cannot produce.
A network of union health funds operating on shared clinical protocols, generating continuous metabolic data across working populations in New York, London, Berlin, Stockholm, and Mumbai, does not just solve a benefits problem. It produces the real-world evidence asset that every major pharmaceutical company developing cardiometabolic drugs needs and cannot generate on its own. The direct-to-employer channel understood one version of this. What it built was a procurement innovation. What the union network makes possible is a production innovation: not just buying care more efficiently, but generating the biological record that makes the next generation of cardiometabolic therapeutics possible, and the regulatory dossier that gets them reimbursed across every major jurisdiction on earth.
The question it opens for every union health fund negotiating benefits for workers in New York City, Stuttgart, Manchester, Mumbai, São Paulo, Istanbul, and Johannesburg is not whether to cover GLP-1 therapy. It is whether to build the clinical protocol infrastructure — the metabolic workup, the continuous monitoring, the outcomes tracking — that converts a cheap generic into a production node in a global biological data network.
Pittsburgh's transformation succeeded, to the extent that it succeeded, with all the wage caveats and labor market limitations that Part I documented, because UPMC understood, before most healthcare systems in the country, that the hospital was not a building. It was a platform.
Thomas Detre, the Hungarian émigré psychiatrist who became UPMC's de facto architect, did not build a better hospital. He built an institution that treated the production of health as an economic export, that looked at the research capacity of the University of Pittsburgh, the clinical depth of its medical center, and the patient base of a post-industrial region and understood that the combination could produce something that people and institutions outside Pittsburgh would pay to access. The organ transplant program. The neurosurgical excellence. The international patient flows that began arriving in the 1990s. These were not accidents. They were the deliberate construction of a clinical platform premium, the systematic conversion of institutional depth into a destination that employers, patients, and eventually insurers would reorganize their behavior around.
New York has everything Pittsburgh had, multiplied by a factor that is difficult to overstate.
What it needs is the Thomas Detre of the cardiometabolic economy, the institutional leader who understands that the production of continuous metabolic health is not a service line or a cost center or a public health initiative. It is an export. It is the thing that people and institutions and AI systems outside New York will pay large sums to access because the depth of the platform — the longitudinal records, the clinical protocols, the research evidence, the manufacturing ecosystems — makes what New York produces worth more than what can be produced anywhere else.
The Imagination Gap
The argument this series is making is not that New York should become a healthcare city. It is already a healthcare city, in the same way Pittsburgh was already a steel city when the mills began closing: deeply, structurally, with a workforce and an institutional identity organized around it.
The Cardiac Borough argument is that being a healthcare city and being a cardiometabolic platform are different things. The difference is the same one that separates having a stock exchange from being the global center of capital markets. One is an institution. The other is a system. One processes transactions. The other sets the terms on which transactions happen everywhere else.
The cardiometabolic platform New York could build would set the terms on which metabolic health is produced, priced, and traded for the next half century.
The clinical protocols developed at Mount Sinai and NYU Langone and NewYork-Presbyterian would become the evidence base that insurers and employers and AI systems around the world build on. The longitudinal metabolic records generated by New York's monitored population would become the training data that makes the next generation of predictive health models possible.
The employer COE contracts negotiated by New York's hospital systems would become the template that other cities and other employers try to replicate, worldwide. The union benefits packages that enroll New York's workers into the metabolic sensing network would become the model that other labor organizations adapt. The manufacturing and distribution infrastructure built around the platform would make New York the node in the cardiometabolic hive whose removal would cost the network more than any other.
On the other hand:
The New York State Senate is now deliberating the Dark Skies Protection Act, a proposed law requiring outdoor lights across New York to shut off at 11pm, a piece of legislation so perfectly calibrated to the current ambitions of the city's political class that it deserves a moment of genuine attention. It will protect migratory birds from disorientation. It will not build the platform. It will not write the union contract that enrolls 185,000 doormen and cleaners into a metabolic sensing network. It will not position New York at the center of the most consequential biological data competition in the history of medicine. It is the kind of policy that happens when leaders run out of larger ideas, when the energy that should be going into the question of what New York builds next is going instead into the question of what New York turns off.
This is what a city looks like when it has exhausted its imagination. Not collapsed, not failed, adrift strategically, just procedurally administering the inventory of its existing assets while the next economy assembles itself in the spaces the city does not know to look at.
The birds will find their way. New York needs to find its nerve.
/ jgs
John G. Singer is the founder and Executive Director of Blue Spoon and the author of When Burning Man Comes to Washington: A Field Manual for Riding Chaos. Hardcore Zen is published weekly on Substack.